The Center for Epidemiologic Studies Depression Scale – Revised (CESD-R) is a 20-item self-report screening instrument designed to assess depressive symptoms and identify individuals who may benefit from further clinical evaluation for major depressive disorder (MDD). Revised from the original CES-D by Eaton et al. (2004), the CESD-R was developed to better align with contemporary diagnostic frameworks while maintaining the efficiency and accessibility of the original scale. This allowed the outcomes of the CESD-R to be applied to the DSM-5 criteria for MDD, creating a powerful tool to aid clinicians.
Respondents rate how frequently they experienced each of the 20 symptoms over the past two weeks using a 5-point frequency scale ranging from “not at all or less than 1 day” to “nearly every day for 2 weeks.”
Sample CESD-R Question

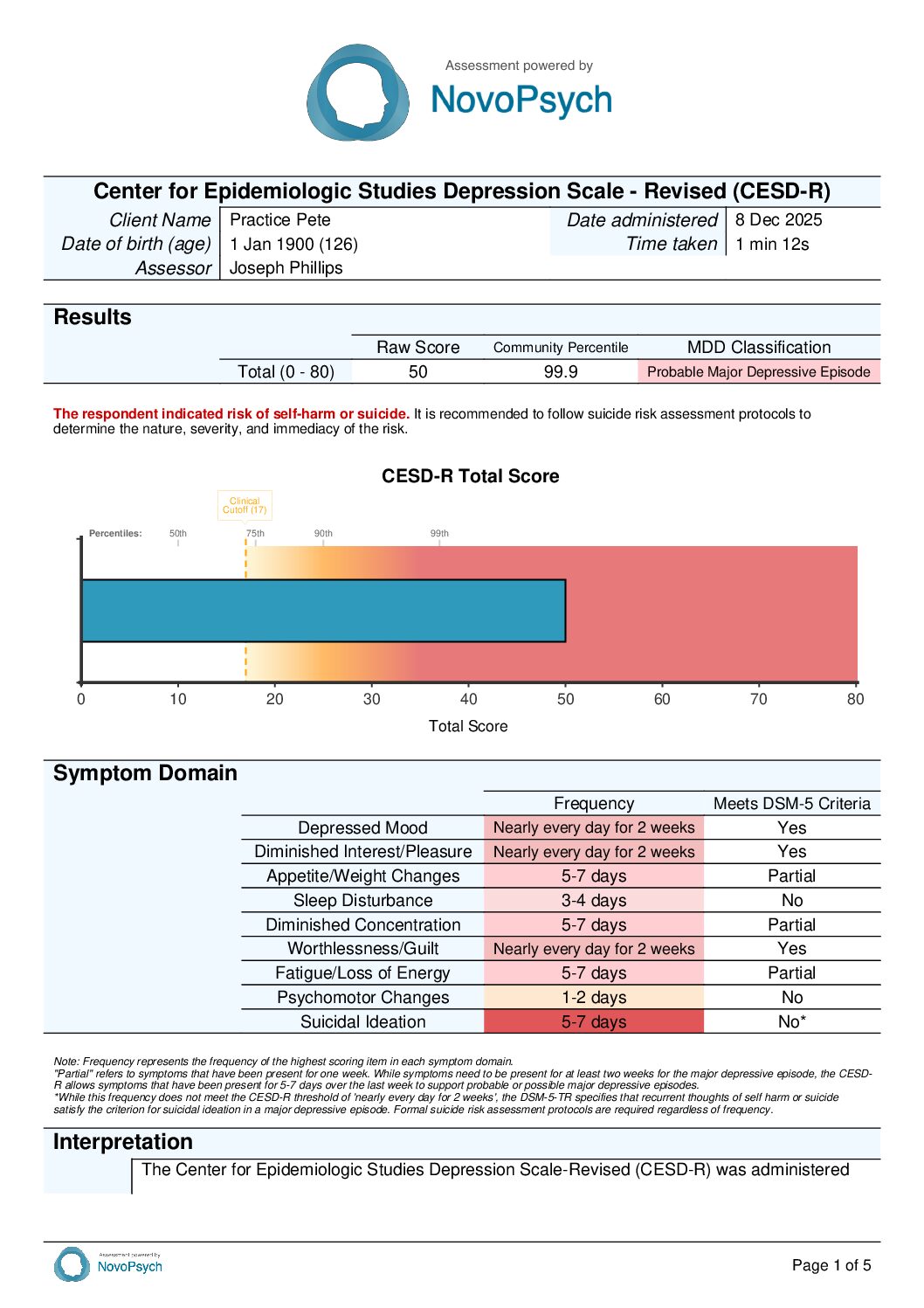
Total scores range from 0 to 80. Lower scores indicate infrequent or absent depressive symptoms, while higher scores indicate more persistent symptom occurrence across multiple domains. A score of 0 represents minimal symptom frequency (symptoms absent or present for less than one day), whereas a score of 80 indicates all symptoms were present nearly every day throughout the two-week assessment period. Administration typically requires 3 minutes to complete, making it practical for use in various clinical settings.
The CESD-R can serve multiple clinical functions. It provides time-efficient initial screening to identify clients who may require comprehensive diagnostic assessment for depression. Repeated administrations track symptom patterns over time (Bean et al. 2024), helping clinicians and clients evaluate intervention effectiveness and identify early warning signs of symptom changes. The symptom domain structure identifies specific areas of concern—such as sleep disturbance, concentration difficulties, or fatigue—allowing clinicians to tailor interventions to individual symptom profiles. Specific items assess self-harm and suicidal ideation with frequency information to inform safety planning and ongoing risk monitoring.
The CESD-R consists of 20 items assessing depressive symptoms, each rated on a 5-point frequency scale. Response options range from 0 (Not at all or less than 1 day) to 4 (Nearly every day for 2 weeks), with higher scores indicating more frequent depressive symptoms. Although the instructions ask respondents to consider symptoms experienced over the “past week or so,” the response options span frequencies of up to two weeks. It is important to note that a response of 0 does not necessarily indicate the absence of a symptom, as it may have been present for less than one day.

The total score ranges from 0 to 80, rather than collapsing the two highest response options (as is sometimes done for comparisons with the original CES-D), which yields a score range of 0-60. This approach is consistent with best practice to support more accurate interpretation across severity levels (Bean et al., 2024). Using this scoring approach, a total score of 17 or greater is proposed as a screening clinical cutoff for clinically significant depressive symptoms (Bean et al., 2024).

The CESD-R uses a DSM-5-informed and empirically evaluated classification system for Major Depressive Disorder (MDD) to aid in identifying individuals requiring comprehensive clinical assessment (Eaton et al., 2012;Van Dam & Earleywine, 2011). It organized items into nine depressive symptom domains:

The CESD-R classifies depression severity using an algorithmic approach that evaluates symptom frequency across nine DSM-5 symptom domains, rather than relying solely on the total score cutoff. For classifications of Meets Criteria, Probable, or Possible Major Depressive Episode, at least one of two core symptoms must be present: depressed mood (dysphoria) or diminished interest/pleasure (anhedonia). The classification level is then determined by the total number of symptom domains endorsed and the frequency with which symptoms occur. For classification purposes, a symptom domain is counted as present if at least one item within that domain meets the required frequency threshold, and qualifying domains—including the core domains—are included in the total domain count. This approach distinguishes DSM-consistent depressive symptom patterns from subthreshold symptom elevations while preserving sensitivity to clinically meaningful presentations. Elevated classifications indicate the need for thorough diagnostic evaluation for MDD.
Classification Levels
The CESD-R allows a lower frequency threshold (5-7 days) for additional symptoms in the ‘Probable’ and ‘Possible’ classifications to enhance screening sensitivity for milder presentations. While DSM-5-TR specifies that suicidal ideation is clinically significant if it has occured on more than one occasion to contribute to an MDD diagnosis, the CESD-R requires 5-7 day frequency for classification purposes. Therefore, clinicians should carefully review responses to the suicidal ideation items (14 & 15), determine if they should count towards establishing a diagnosis of MDD, and consider whether a risk assessment is warranted.
When the CESD-R is administered repeatedly to track symptom changes over time, a Minimally Important Difference (MID) threshold of 6 points distinguishes clinically meaningful change from normal measurement variability. Score changes of 6 points or greater (either increase or decrease) represent clinically meaningful worsening or improvement, while changes below this threshold may suggest stability or fluctuations that do not reach clinical significance.
Multiple validation studies support a unidimensional factor structure for the CESD-R. Van Dam and Earleywine (2011) conducted confirmatory factor analysis in both a large community sample (N = 7,389) and a student sample (N = 245), finding strong factor loadings ranging from 0.49 to 0.86. Bean et al. (2024) confirmed essential unidimensionality through bifactor analysis, with the general factor showing correlations of 0.93-0.94 to the one-factor model. These converging findings across multiple samples provide robust support for treating the CESD-R as a unidimensional measure of depression severity.
The CESD-R demonstrates excellent internal consistency across multiple studies and populations. Van Dam and Earleywine (2011) reported Cronbach’s alpha of 0.923 in their community sample (N = 7,389) and 0.93 in their student sample (N = 245). These high reliability coefficients indicate that the scale items consistently measure the same underlying construct.
Sriken et al. (2024) replicated these findings in their university sample, reporting excellent internal consistency for the total score (α = 0.92). Kimong et al. (2023) conducted a comprehensive psychometric synthesis of 18 CESD-R studies in English, reporting an aggregated internal consistency of α = 0.92, demonstrating excellent and consistent score reliability across diverse samples. This meta-analytic finding provides strong evidence for the scale’s reliability as a screening instrument.
Bean et al. (2024) reported Cronbach’s alpha of 0.95 for both the 4-point and 5-point response option versions, along with McDonald’s omega values of 0.95, further confirming the scale’s excellent internal consistency.
Convergent: The CESD-R shows expected relationships with theoretically related constructs. Depression commonly co-occurs with anxiety and is characterized by high negative affect and low positive affect (Mineka, Watson & Clark, 1998). Van Dam and Earleywine (2011) found moderate to strong positive correlations with the State-Trait Inventory for Cognitive and Somatic Anxiety (STICSA) and expected patterns with the Positive and Negative Affect Schedule (PANAS), including correlations with negative affect and inverse relationships with positive affect. Sriken et al. (2024) found a strong correlation with the Generalized Anxiety Disorder-7 (GAD-7; r = 0.67).
Discriminant: The CESD-R shows appropriate independence from unrelated constructs, confirming it measures depression specifically rather than general distress or other pathologies. Van Dam and Earleywine (2011) found appropriately modest correlations with the Schizotypal Personality Questionnaire-Brief (SPQ-B), indicating the scale measures depression distinctly from schizotypy. Sriken et al. (2024) demonstrated minimal correlation with the Alcohol Use Disorders Identification Test (r = 0.12) and Social Justice Scale (r = 0.02).
The CESD-R has also been validated across diverse populations, with measurement invariance demonstrated across gender and ethnic groups in the United States (Sriken et al., 2024), and translations available in at least twelve languages showing preliminary validation evidence.