A child self-report version of the same measure (MFQ-self) is also available, and the two measures can be used in combination. The MFQ-Parent was created as an abbreviated version of the 33-item Mood and Feelings Questionnaire to provide a brief, psychometrically sound instrument suitable for clinical screening. The MFQ-Parent has been recommended by the National Institute for Health and Clinical Excellence (NICE) guidelines as a screening tool for childhood and adolescent depression (Middleton et al., 2005). Using the parallel, self-report version version together with the MFQ-Parent can give a clearer picture of the youth’s symptoms at home and in daily life.
MFQ-Parent Example Item

While the MFQ-Parent is commonly referred to as the Short Mood and Feelings Questionnaire – Parent (SMFQ-P) in the literature, NovoPsych uses the abbreviated name, MFQ-Parent, throughout this report. The MFQ-Parent was designed based on DSM diagnostic classifications (Angold et al., 1995). While there are no subscales, items assess a range of cognitive and affective components of depressive symptoms, including negative self-evaluation, low mood, and anhedonia, whilst also capturing symptoms of tiredness, restlessness, and poor concentration (Sharp et al., 2006; Thabrew et al., 2018; Turner et al., 2014).
Depression is a significant public health concern amongst young people, affecting up to one in five youth before reaching 18 years of age (Lewinsohn et al., 1993). Youth-onset depression is particularly concerning due to its association with poorer educational attainment, impaired interpersonal relationships and increased risk of recurrence in adulthood (Copeland et al., 2009; Hammen et al., 2008). The MFQ-Parent addresses a critical need for efficient depression screening in clinical and research settings, as comprehensive diagnostic interviews are time-intensive and may not be feasible for large-scale screening programmes.
The MFQ-Parent can be used to aid clinicians in multiple ways within comprehensive mental health care, including initial screening to identify youth who may require diagnostic evaluation and further assessment. It also serves as a valuable tool for tracking symptom changes during treatment, with research demonstrating sensitivity to therapeutic interventions (Thabrew et al., 2018). The MFQ-Parent can also support treatment planning by providing a quantifiable baseline of symptom severity and by identifying specific symptom domains warranting clinical attention. For instance, elevated scores on items assessing concentration difficulties and tiredness may suggest the need for psychoeducation about sleep hygiene, whilst high scores on items related to negative self-evaluation may indicate that cognitive restructuring would be beneficial.
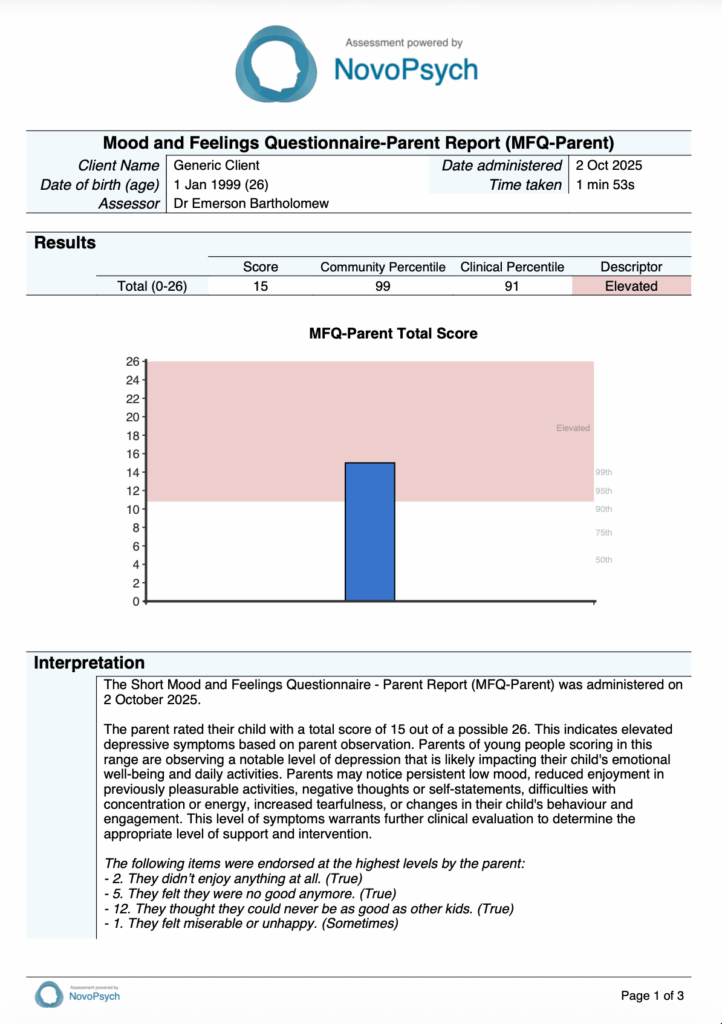
Each of the 13 MFQ-Parent items are scored 0 (not true), 1 (sometimes), or 2 (true), reflecting the frequency of depressive symptoms observed in the child over the past 2 weeks. The sum of responses to all items produces a total score ranging from 0 to 26. Higher scores indicate greater severity of depressive symptoms.

The established total cut-off score of 11 and above indicates the presence of significant depressive symptoms that warrant further evaluation. This threshold was established by Thapar and McGuffin (1998) and demonstrates good sensitivity and specificity for identifying youth with depressive disorders. The total score is also presented in comparison to a community sample of children (aged 6-8), and a clinical sample (aged 11-13) who met diagnostic criteria for depression.
The MFQ-Parent can be used for monitoring symptom changes over time during treatment. Research examining meaningful score changes suggests a 2-point change in either direction represents a noticeable shift in symptom severity.
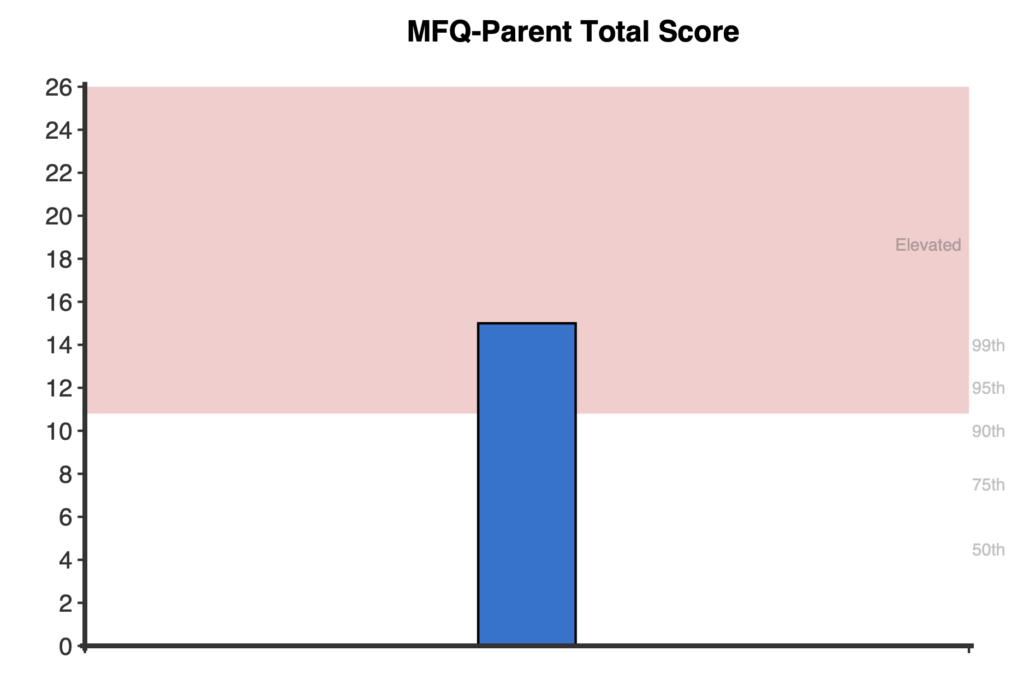
On first administration, a bar graph displaying the total raw score is presented.
When the assessment is administered multiple times, a longitudinal line graph is generated to track changes in the total raw score over time.

The MFQ-Parent demonstrates strong construct validity through multiple lines of evidence. The scale shows robust convergent validity with other measures of depression and related constructs. Strong correlations have been observed with measures of emotional symptoms and anxiety across multiple validation studies (Fernández-Martínez et al., 2020). Research examining associations with external validators found significant correlations with anxiety symptoms and emotional difficulties, supporting the scale’s ability to capture clinically meaningful variation in depressive symptomatology.
The MFQ-Parent exhibits excellent internal consistency across diverse samples and age groups. Cronbach’s alpha coefficients consistently fall within the good to excellent range, including α = .83 in a community sample of 6-8 year olds (Fernández-Martínez et al., 2020) and α = .80 to .91 in various samples aged 6 to 17 years (Angold et al., 1995). Test-retest reliability over an eight-week period has been demonstrated with an intraclass correlation coefficient of .80, indicating stable measurement of depressive symptoms over time (Fernández-Martínez et al., 2020).
The MFQ-Parent has been extensively validated as a unidimensional measure. Confirmatory factor analyses consistently support a single-factor structure across development, from early school age through adolescence (Fernández-Martínez et al., 2020; Thabrew et al., 2018). The robust unidimensional structure provides strong justification for using sum scores in clinical contexts.
Criterion validity has been established through numerous studies examining the MFQ-Parent’s ability to discriminate between depressed and non-depressed youth. Across samples aged 6 to 17 years, the scale demonstrates acceptable to good sensitivity ranging from .60 to .86, specificity from .61 to .87, and discrimination ability with area under the curve (AUC) values of .72 to .84 when compared against structured clinical interviews (Angold et al., 1995; Rhew et al., 2010; Thapar & McGuffin, 1998). The scale also demonstrates sensitivity to change following treatment, making it a valuable tool for monitoring symptom changes over time during treatment.
Normative data for the MFQ-Parent have been reported across multiple samples. Community normative data are derived from Fernández-Martínez et al. (2020), who examined the MFQ-Parent in a Spanish community sample of children aged 6-8 years (N = 181). This sample demonstrated a mean total score of 4.59 (SD = 4.27). The clinical comparison group was derived from Rhew et al. (2010), who validated the MFQ-Parent in a sample of young adolescents (N = 521, mean age 11.5 years). The depressed subsample had a mean total score of 7.3 (SD = 5.8) and included youth meeting diagnostic criteria for depression. These samples provide valuable comparison groups for interpreting scores.
Thapar and McGuffin (1998) established a cut-off of 11 or above to indicate clinically significant depressive symptoms. This cut-off has demonstrated good sensitivity and specificity for identifying youth with depressive disorders and provides a useful threshold for understanding depression severity.