MAIA-2 Overview
MAIA-2 Scoring & Interpretation
MAIA-2 Psychometrics
MAIA-2 Overview
Multidimensional Assessment of Interoceptive Awareness – Version 2 (MAIA-2) General Overview
Interoception refers to the body’s ability to sense what is happening internally. This may include heart rate, breathing, hunger, temperature, pain, and the bodily sensations associated with emotional experiences. It operates across both conscious and unconscious levels, providing an ongoing representation of the body’s state (Khalsa et al., 2018). Interoceptive awareness refers specifically to the conscious perception of these internal signals, including how individuals attend, interpret, and regulate them, as well as how they make sense of the thoughts and feelings that arise in response (Mehling et al., 2012).
The MAIA-2 comprises eight subscales, each capturing a distinct facet of the interoceptive awareness construct (Mehling et al., 2012):
- Noticing: Awareness of uncomfortable, comfortable, and neutral body sensations, representing the basic sensory dimension of body awareness.
- Not-Distracting: The tendency not to ignore or distract oneself from sensations of pain or discomfort.
- Not-Worrying: Captures the degree to which a person can experience sensations of pain or discomfort without emotional distress or worry.
- Attention Regulation: Ability to sustain and control attention to body sensations, including the capacity to maintain and return attention to bodily sensations, even in the presence of distraction.
- Emotional Awareness: Awareness of the connection between body sensations and emotional states, reflecting recognition of how emotions are experienced as bodily changes.
- Self-Regulation: Ability to regulate psychological distress by attending to and engaging with body sensations to promote calm or stability.
- Body Listening: Active listening to the body for insight, including attending to bodily signals for information about emotional state and what to do.
- Trusting: The experience of one’s body as safe and trustworthy, reflecting a felt sense that the body is a reliable place.
Example MAIA-2 Item

Clinical Application of the MAIA-2
The MAIA-2 is not a diagnostic instrument, and its eight subscales allow clinicians to identify specific strengths and difficulties in a client’s body awareness profile. It is best used as a multidimensional progress monitoring and outcome measure, with higher interoceptive awareness scores generally reflecting more adaptive ways of attending to and interpreting bodily signals, which have been associated with improved wellbeing, emotional regulation, and reduced maladaptive responding (Solano Durán et al., 2024). From a clinical perspective, in most clinical contexts higher scores on the MAIA-2 subscales can be interpreted as strengths in adaptive interoceptive awareness and self-regulation that may be leveraged to support therapeutic intervention.
In general, low scores on MAIA-2 subscales reflect reduced conscious awareness of, or adaptive engagement with, internal body signals, whether through limited detection of sensations, avoidance of discomfort, or difficulty using bodily information to guide behaviour. For example, low Trusting and Not-Worrying have been observed in depressed individuals, and diminished Trusting has been found to be the most consistent interoceptive correlate of suicidal ideation (Eggart et al., 2021; Solano Durán et al., 2024). However, low scores on individual subscales do not always tell the full story. Clinicians should also consider the pattern of scores across the profile. For example, elevated scores on awareness-related subscales (Noticing, Emotional Awareness, Body Listening) combined with low scores on regulatory or tolerance subscales (Not-Distracting, Not-Worrying, Trusting) may indicate that heightened body awareness is experienced as distressing rather than adaptive, as has been observed in individuals with disordered eating (Mensinger et al., 2025).
The MAIA-2 is particularly relevant in contexts involving mindfulness-based and mind-body interventions, chronic pain management, and trauma-informed treatment, where interoceptive awareness and bodily awareness are therapeutic targets (Price & Hooven, 2018). Beyond these contexts, the MAIA-2 has also been used in research and clinical settings with populations including eating disorders, depression, anxiety, autism spectrum disorder, and chronic pain, with different patterns of subscale scores showing relevance across conditions (Solano Durán et al., 2024).
MAIA-2 Scoring & Interpretation
Scoring the Multidimensional Assessment of Interoceptive Awareness – Version 2 (MAIA-2)
Each item is rated from 0 (Never) to 5 (Always), with some items reverse-scored. Scoring consists of calculating the average score for each of the eight subscales (sum of responses to the items in the subscale divided by the number of items, then rounded to 2 decimal places). The resulting subscale score ranges from 0 to 5, where higher scores indicate greater interoceptive awareness in that dimension.
There is no total score calculated as higher scores do not uniformly indicate better outcomes across all subscales, and the pattern of scores across the profile is often more clinically informative than any individual subscale score. For example, elevated Noticing combined with low Not-Worrying may reflect distress rather than adaptive awareness. A total score would collapse these clinically important distinctions into a single number.
MAIA-2 Results Table
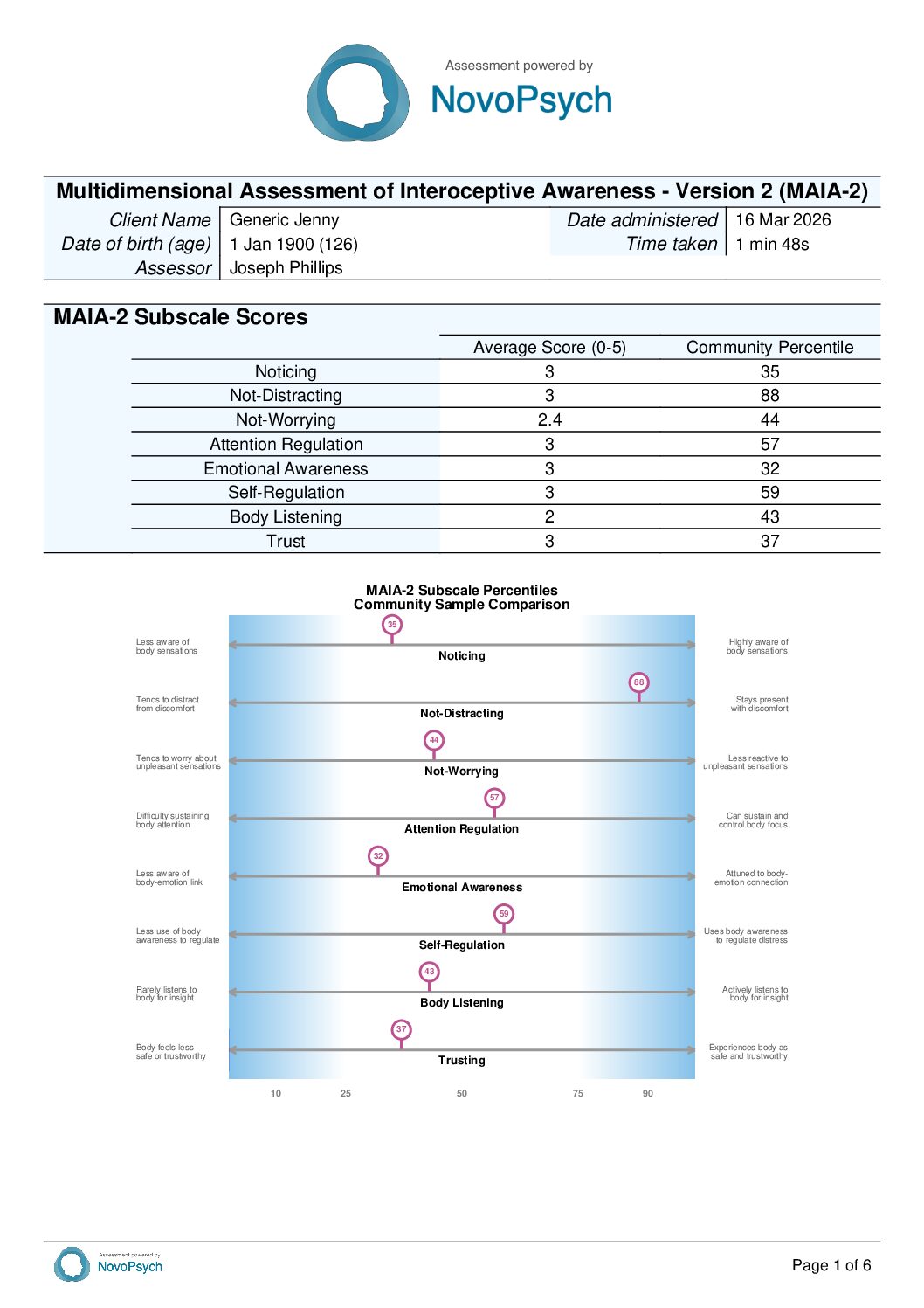
Results are presented in a summary table reporting each subscale average score and corresponding community percentile.

Interpreting MAIA-2 Subscales
For all MAIA-2 subscales, higher scores indicate greater interoceptive awareness, generally reflecting adaptive capacities. Items marked (R) are reverse-scored. Low scores may be particularly clinically informative, as they can indicate reduced body awareness, avoidant coping, or a disrupted relationship with bodily experience.
While higher scores generally reflect more adaptive interoceptive functioning, scores should be interpreted in the context of the full subscale profile. The pattern of scores across subscales is often more clinically informative than any individual score considered in isolation.
- Noticing (Items 1, 2, 3, 4): Awareness of uncomfortable, comfortable, and neutral body sensations. A low score suggests the individual may have limited conscious awareness of what is happening in their body, potentially resulting in difficulties recognising early signs of stress, fatigue, or emotional shifts. A high score may indicate strong sensory awareness of bodily states, though in some individuals this may co-occur with heightened vigilance to physical sensations.
- Not-Distracting (Items 5(R), 6(R), 7(R), 8(R), 9(R), 10(R)): Tendency not to ignore or distract from sensations of pain or discomfort. A low score suggests the individual may tend to suppress or avoid uncomfortable body signals rather than attending to them, which may limit their capacity to use bodily information adaptively. A high score indicates a willingness to stay present with discomfort rather than turning away from it.
- Not-Worrying (Items 11(R), 12(R), 13, 14, 15(R)): Tendency not to worry or experience emotional distress with sensations of pain or discomfort. A low score suggests the individual may become emotionally distressed when they notice uncomfortable physical sensations, potentially amplifying pain or anxiety through worry. A high score indicates the ability to notice discomfort without it triggering an escalating emotional response.
- Attention Regulation (Items 16, 17, 18, 19, 20, 21, 22): Ability to sustain and control attention to body sensations. A low score suggests difficulty deliberately directing, holding, or shifting attention to bodily signals, which may limit the use of body-based coping strategies. A high score indicates the individual can intentionally focus on, broaden, or redirect their bodily attention as needed.
- Emotional Awareness (Items 23, 24, 25, 26, 27): Awareness of the connection between body sensations and emotional states. A low score suggests the individual may have difficulty recognising how emotions manifest physically, which may present as alexithymia or difficulty labelling emotional states. A high score indicates strong awareness that body sensations and emotions are connected, though in some presentations this may be accompanied by heightened sensitivity to the physical aspects of anxiety.
- Self-Regulation (Items 28, 29, 30, 31): Ability to regulate psychological distress by attending to body sensations. A low score suggests the individual may not use body awareness as a tool for managing distress, for example, using breath to reduce tension or calm down, and may represent a useful target for therapeutic intervention. A high score indicates the individual may actively draw on bodily attention to regulate their emotional state.
- Body Listening (Items 32, 33, 34): Active listening to the body for insight and decision-making. A low score suggests the individual may not generally consult their body for information when making decisions or trying to understand how they feel. A high score indicates they may actively seek out and use bodily signals to guide their responses and choices.
- Trusting (Items 35, 36, 37): Experience of one’s body as safe and trustworthy. A low score suggests the individual may not feel at home in their body, or may experience their body as unreliable or threatening. This may be particularly relevant in trauma, chronic pain, and depersonalisation presentations. A high score indicates a felt sense of safety and reliability in one’s bodily experience.
MAIA-2 Percentiles
Each MAIA-2 subscale average score is converted to a community percentile, indicating how a respondent’s score compares with the general population. A percentile of 50 means the respondent scored at the community sample average on that subscale, while a percentile of 75 means they scored higher than 75% of the community sample. Percentiles are interpreted as follows: low (below the 25th percentile), average (25th to 75th percentile), and high (above the 75th percentile).
Scores within the average range indicate that the respondent’s interoceptive awareness on that facet is broadly comparable to the general population and is unlikely to require specific clinical attention. The MAIA-2 is most clinically informative at the extremes of the distribution, where scores fall outside the average range. Low scores may point to reduced body awareness or avoidant patterns that are relevant to case formulation, while high scores may reflect strengths that can be leveraged therapeutically, or in some profiles, heightened sensitivity that warrants further exploration.
MAIA-2 Single Administration Graph
For single administrations, a horizontal chart displays each subscale’s community sample percentile along a 0–100 axis, with shaded regions below the 25th and above the 75th percentile highlighting scores outside the average range. This provides a visual profile of interoceptive awareness relative to the normative sample.

MAIA-2 Multi-timepoint Graph
For multiple administrations, each subscale is presented as a separate line graph plotting average scores over time. These allow clinicians to observe changes in each and monitor progress during treatment.
![]()
MAIA-2 Psychometrics
Development and Factor Structure of the Multidimensional Assessment of Interoceptive Awareness – Version 2 (MAIA-2)
The MAIA-2 is a revised version of the original 32-item MAIA (Mehling et al., 2012). Poor internal consistency in two subscales (Not-Distracting and Not-Worrying) was improved by adding five items, bringing the total to 37 items and reflecting a revised eight-factor structure (Mehling et al., 2018).
Reliability and Validity of the MAIA-2
Internal consistency across most MAIA-2 subscales is acceptable, with Cronbach’s alphas ranging from .64 (Noticing) to .83 (Attention Regulation, Trusting) in a community sample. The lower alpha for Noticing is consistent with its brevity (4 items) and aligns with values reported across validation studies (Mehling et al., 2012; 2018). In a clinical sample of patients with major depressive disorder (N = 110; Eggart et al., 2021), reliability improved over the course of treatment, and all eight subscales demonstrated sensitivity to clinical change, with improvements associated with reductions in depression severity. Test-retest reliability data for the MAIA-2 are currently limited.
Normative Data and Percentile Rankings of the MAIA-2
Percentile rankings for each MAIA-2 subscale are derived from the community normative sample reported in Mehling et al. (2018), comprising 1,090 adults (mean age 30.6 years, SD = 11.3). Percentiles are calculated from the reported mean and standard deviation for each subscale, under the assumption of an approximately normal distribution. A percentile of 50 indicates a score at the community sample average.
Normative (community sample) means and standard deviations for MAIA-2 subscales (Mehling et al., 2018):
- Noticing: M = 3.34, SD = 0.90
- Not-Distracting: M = 2.06, SD = 0.80
- Not-Worrying: M = 2.52, SD = 0.85
- Attention Regulation: M = 2.84, SD = 0.86
- Emotional Awareness: M = 3.44, SD = 0.96
- Self-Regulation: M = 2.78, SD = 1.01
- Body Listening: M = 2.20, SD = 1.17
- Trusting: M = 3.37, SD = 1.11
Assess your patients with the Multidimensional Assessment of Interoceptive Awareness – Version 2 using a NovoPsych account
- For Psychologists & Mental Health Clinicians
- Send Assessments to Patient’s Phone
- Receive Comprehensive Reports
- Access Over 100 Validated Assessments
- Instant Psychometric Scoring
- Track Symptoms
- Inform Treatment


Download MAIA-2 PDF
MAIA-2 Sample Results
