Social support represents a fundamental protective factor for psychological wellbeing, with extensive research demonstrating its buffering effects against stress, depression, and various mental health challenges. The theoretical framework underlying the Brief 2-Way SSS recognises that social support operates as a reciprocal process, where both providing and receiving support contribute meaningfully to wellbeing outcomes. This bidirectional conceptualisation moves beyond traditional unidirectional models that primarily focus on support receipt, acknowledging the psychological benefits individuals derive from being support providers themselves. While the measure assesses perceived rather than objectively measured support exchanges, research indicates that subjective perceptions of support may be more crucial for psychological wellbeing than actual support received (Haber et al., 2007).
Example Brief 2-Way SSS Item

The scale measures both instrumental (tangible practical support), and emotional support (the presence of empathy, concern, affection and encouragement) across both giving and receiving, covering four distinct dimensions:
Research demonstrates that the scale shows relationships with wellbeing indicators, with higher scores associated with greater life satisfaction and general health, and negatively associated with perceived stress and depression. Notably, the giving support dimensions demonstrate unique predictive value beyond receiving support alone, underscoring the psychological benefits of being a support provider, not merely a recipient.
Clinically, the Brief 2-Way SSS serves multiple assessment functions. During initial assessment, it provides insight into clients’ social resources and potential areas of social deficit that may contribute to psychological distress. The scale’s bidirectional nature allows clinicians to identify not only whether clients feel adequately supported, but also whether they have opportunities to provide support to others, a factor increasingly recognised as important for psychological wellbeing and sense of purpose. For formulation purposes, understanding patterns across the four dimensions can inform targeted interventions. For instance, a client scoring low on giving support dimensions might benefit from volunteer opportunities or structured ways to contribute to their community, whilst deficits in receiving instrumental support might indicate practical resource needs.
The scale proves particularly valuable in assessing older adults, individuals experiencing social isolation, those adjusting to major life transitions, and clients presenting with mood or anxiety disorders where social support represents a key maintaining or protective factor. Its behavioural anchoring, asking about specific supportive actions rather than abstract perceptions, provides concrete targets for intervention planning.
A total score ranging from 0-60 and subscale scores ranging from 0 to 15 are provided, with higher scores indicative of higher levels of social support. Subscales are comprised of the following items:
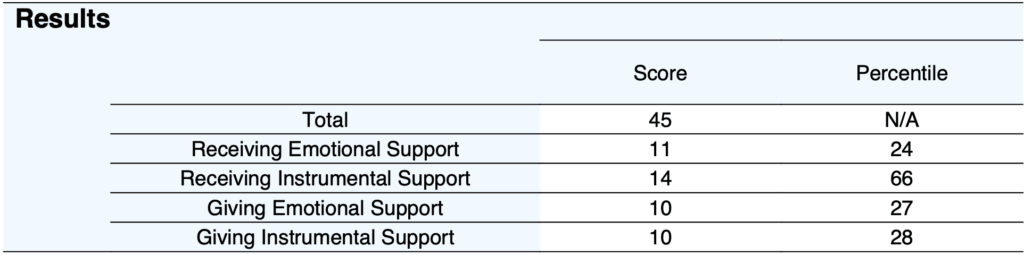
Percentile ranks are presented which compare the respondent’s scores to a normative sample of older adults (aged 55 plus, Obst, et al 2019). A percentile of 50 represents average levels of social support, whereas a percentile of 10 indicates a level of social support which is in the bottom 10 percent compared to older adults. Given some positive skew in normative distributions, percentile interpretation should consider that scores cluster toward the higher end, making lower scores particularly clinically significant. No total score percentile is reported as no total mean and standard deviation was reported by Obst et al. (2019).

For clinical interpretation, examining patterns across subscales is particularly informative. Balanced profiles with similar scores across all four dimensions suggest well-integrated reciprocal support relationships. Large discrepancies between giving and receiving dimensions may indicate relationship imbalances warranting exploration. For instance, high receiving but low giving scores might suggest dependency patterns or limited opportunities for contribution, whilst the reverse pattern could indicate caregiving burden or difficulty accepting help. A second results table shows a ratio representing the difference between giving and receiving support (giving minus receiving) for total, instrumental and emotional. A positive score indicates more support given than received, while a negative score indicates they receive more support than they provide. A score near zero suggests balance.
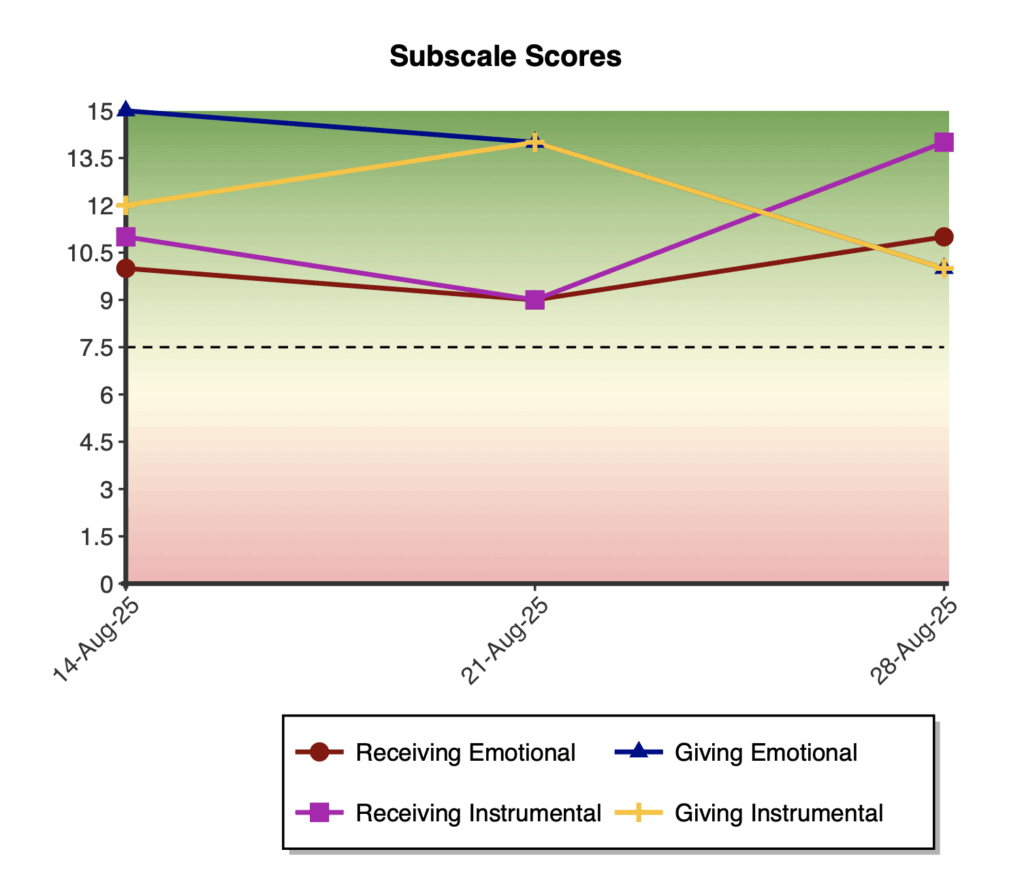
On first administration a bar graph of subscale raw scores is presented, with a threshold of 7.5 as an indicator of halfway between 15 and 0.

On multiple administrations, two line graphs are shown for the total and the subscale scores over time.

The scale demonstrates strong construct validity through both convergent and divergent validity evidence. Convergent validity is supported through significant positive correlations with established social support measures, including the Social Support Questionnaire (r = .42-.55 for receiving dimensions) and the Berlin Social Support Scale (r = .62-.66 for receiving dimensions). The receiving emotional support subscale shows the strongest associations with these existing measures, which is expected given their primary focus on emotional support receipt. Incremental validity is evident through the scale’s ability to predict unique variance in wellbeing outcomes beyond existing unidirectional support measures, with the four subscales accounting for significant incremental variance in depression (ΔR² = .036), perceived stress (ΔR² = .05), and life satisfaction (ΔR² = .064) after controlling for traditional support measures.
Reliability analyses consistently demonstrate good to excellent internal consistency across diverse samples. In the original validation with Australian older adults, Cronbach’s alpha coefficients ranged from α = .75 for giving instrumental support to α = .88 for receiving emotional support at Time 1, with similar values at 3-month follow-up (α = .77-.90) (Obst et al., 2019). In a separate study, McDonald’s omega coefficients ranged from ω = .82 to ω = .91 across subscales, with an overall scale reliability of ω = .88 (Khodabakhsh & Tan, 2022). Test-retest reliability over three months showed stability coefficients ranging from r = .66 to r = .77, indicating good temporal stability whilst allowing for genuine change in support patterns.
Factor analytic studies consistently support the scale’s four-factor structure. Initial confirmatory factor analysis with Australian older adults (n = 306) demonstrated excellent fit for the hypothesised second-order model with two higher-order factors (receiving and giving support) and four first-order factors (χ²/df = 1.37, CFI = .99, TLI = .98, RMSEA = .04, SRMR = .04) (Obst et al., 2019). Cross-cultural validation with Malaysian older adults (n = 249) found optimal fit for a second-order model with one general social support factor and four first-order dimensions (CFI = 1.00, TLI = 1.02, RMSEA = .00, SRMR = .04), suggesting cultural variations in the hierarchical conceptualisation whilst maintaining the fundamental four-dimension structure (Khodabakhsh & Tan, 2022).
Normative data is reported from Obst et al. (2019) in a sample of Australian older adults (n = 306).



