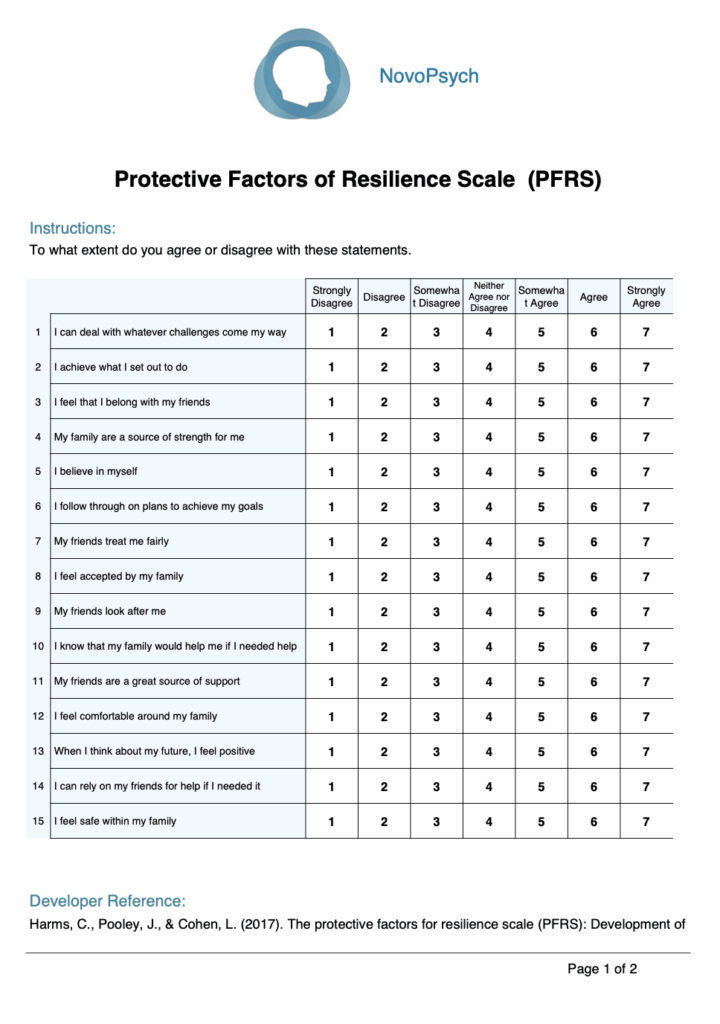
Rather than conceptualising resilience as an outcome or trait, the PFRS measures resilience as a constellation of internal and external resources that can be accessed during times of stress. The scale was developed based on Pooley and Cohen’s (2010) definition of resilience, which emphasises “the potential to exhibit resourcefulness by using available internal and external resources in response to different contextual and developmental challenges.”
The theoretical framework underlying the PFRS draws from resilience research identifying three overarching protective categories: attributes of the individual, aspects of family support, and characteristics of the wider social environment (Garmezy, 1987; Rutter, 1987; Werner & Smith, 1992). The scale operationalises these domains through three distinct subscales:
Clinically, the PFRS serves multiple functions. It can identify existing protective resources that can be leveraged during treatment, assess which resource domains may need strengthening, and guide the development of targeted interventions based on specific resource deficits. For example, an individual with strong personal resources but limited family support might benefit from interventions focused on building alternative support networks or addressing family dynamics. The scale is also valuable for providing a strengths-based complement to deficit-focused assessments.
A total score is given ranging from 15 to 105, with higher scores indicating greater protective resources for resilience.
Three subscale scores are be calculated each ranging from 5-35:
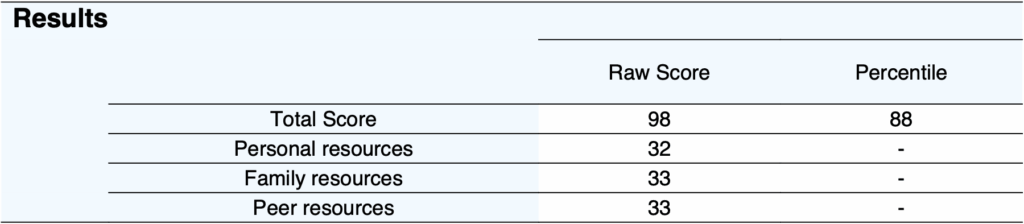
Based on the normative sample (M = 78.90, SD = 15.98), percentile rankings can be calculated to contextualise individual scores. A score at the 50th percentile (approximately 79) represents typical protective resources in the general adult population.
The PFRS is particularly valuable when integrated with comprehensive clinical assessment, providing a strengths-based perspective to complement traditional symptom-focused measures. High scores should not be interpreted as immunity to psychological difficulties but rather as indicating available resources that can be mobilised during treatment. Conversely, low scores highlight specific areas where building protective resources might enhance treatment outcomes and long-term resilience.

On first administration a bar graph of the three subscales is shown with green and red gradients around the top and bottom 30% areas indicating greater or lesser resources for resilience. On multiple administrations, the same bar graph is produced alongside a line graph of the total percentile to track changes over time.

The scale demonstrates robust psychometric properties across multiple validation studies. Construct validity has been extensively examined through both convergent and divergent validity approaches. The scale shows strong positive correlations with measures of wellbeing and adaptive functioning, including significant associations with self-esteem (r = .57, p < .01), life satisfaction (r = .58, p < .01), and having both emotional and instrumental support available (Harms et al., 2017). Divergent validity is supported through negative correlations with maladaptive outcomes, including self-blame (r = -.40, p < .01), substance use (r = -.19, p < .01), and behavioural disengagement (r = -.37, p < .01).
The PFRS also demonstrates meaningful relationships with coping strategies, providing further evidence of construct validity. Individuals reporting higher protective resources showed greater use of adaptive coping strategies including emotional and instrumental support-seeking (r = .35, p < .01), positive reframing and acceptance (r = .27, p < .01), while showing reduced reliance on maladaptive strategies such as self-blame and distraction (r = -.40, p < .01) and behavioural disengagement (r = -.37, p < .01). These patterns support the theoretical proposition that protective resources facilitate adaptive responses to stress.
Internal consistency for the PFRS is excellent, with Cronbach’s alpha values ranging from α = .81 to .93 across different samples. The total scale reliability was α = .93 in the initial validation study (n = 413), while individual subscales demonstrated good to excellent reliability: Personal Resources (α = .85-.92), Family Resources (α = .86-.91), and Peer Resources (α = .80-.89). These reliability coefficients have been replicated across multiple independent samples, supporting the scale’s consistency across diverse populations.
The factor structure of the PFRS has been confirmed through both exploratory and confirmatory factor analyses. The initial exploratory factor analysis (Stage 1, n = 413) revealed a clear three-factor structure explaining 66.13% of the total variance. This structure was subsequently validated through confirmatory factor analysis (Stage 2, n = 240), which supported a second-order factor model where a single overarching resilience factor explained the associations between the three lower-order factors. The model demonstrated good fit indices: CFI = .99, SRMR = .05, and RMSEA = .057 (90% CI = .042-.071).
Importantly, the second-order factor model provides empirical justification for calculating a total PFRS score alongside subscale scores, addressing a common limitation in resilience measurement where summing subscale scores lacks statistical support. The second-order factor loadings were substantial: Personal Resources = .64, Peer Resources = .73, and Family Resources = .66, indicating that while each subscale captures unique variance, they collectively contribute to an overarching protective resource construct.
Normative data is available based on a North American adult sample (n = 240; 58.6% female, M age = 35.34, SD = 11.32 years). The mean total score was 78.90 (SD = 15.98). While means and standard deviations were not reported for individual subscales in the original publication, the total score normative data enables calculation of percentile rankings for clinical comparison. The scale shows a slight negative skew in community samples, indicating that most individuals report moderate to high levels of protective resources, which aligns with resilience theory suggesting that protective factors required for adaptation are not extraordinary but rather consist of normative developmental resources.