Developed as a modification of the North Carolina Family Assessment Scale (NCFAS), the SAS was specifically adapted to capture the nuanced interplay between family strengths and challenges that characterise complex child welfare cases (Kirk & Reed-Ashcraft, 2001). The scale employs a bidirectional rating system that acknowledges families’ capacities alongside their vulnerabilities, providing a balanced framework for assessment and intervention planning.
SAS Example item
The theoretical foundation of the SAS rests on ecological systems theory and strength-based approaches to child welfare practice (Bronfenbrenner & Morris, 2006; Walsh, 2002). This dual focus recognises that families involved with child protection services typically present with both protective factors that can be leveraged and risk factors requiring intervention. The scale is intended for use by qualified clinicians who have sufficient familiarity with the family through direct observation, case records, or collaborative information from multiple sources.
The SAS comprises six distinct domains that comprehensively evaluate family functioning:
Research has demonstrated the SAS’s utility in distinguishing between different types of maltreatment, with particular sensitivity to physical abuse compared to neglect (Berry et al., 2003). The scale’s bidirectional scoring system, ranging from serious stressors to clear strengths, enables practitioners to identify specific intervention targets whilst maintaining awareness of existing family resources and protective factors (Blair et al., 2009).
In clinical practice, the SAS serves multiple functions within child protection services. Practitioners utilise the instrument during initial assessments to develop comprehensive family profiles that inform case planning decisions (U.S. Department of Health and Human Services, 2018). The scale’s domain structure facilitates targeted intervention planning by highlighting specific areas requiring support whilst acknowledging existing family strengths that can be incorporated into treatment approaches. For instance, a family demonstrating clear strengths in social support but significant stressors in parental capabilities might benefit from interventions that leverage their support network to enhance parenting skills through peer mentoring or supported playgroups. The SAS also functions as an outcome monitoring tool, with repeated administrations documenting family progress and informing decisions about service intensity, case closure, or alternative permanency planning.
The scale uses a 6-point rating scale for each item, ranging from -3 to +2, where negative scores indicate stressors and positive scores represent strengths. This asymmetric scale acknowledges that risk factors may require more nuanced differentiation than protective factors in child protection contexts. Items within each domain are summed to produce raw scores, which are then averaged to generate domain-level scores maintaining the -3 to +2 range.

Higher positive scores across domains suggest family resilience and capacity, whilst negative scores highlight vulnerabilities and risks. The scale does not produce a total score, encouraging practitioners to maintain focus on the unique profile of strengths and challenges within each family rather than reducing complex family dynamics to a single risk indicator. This domain-specific approach facilitates targeted intervention planning and enables practitioners to track differential progress across various aspects of family functioning over time.
Domain raw score ranges:
Interpretation guidelines for averaged domain scores:
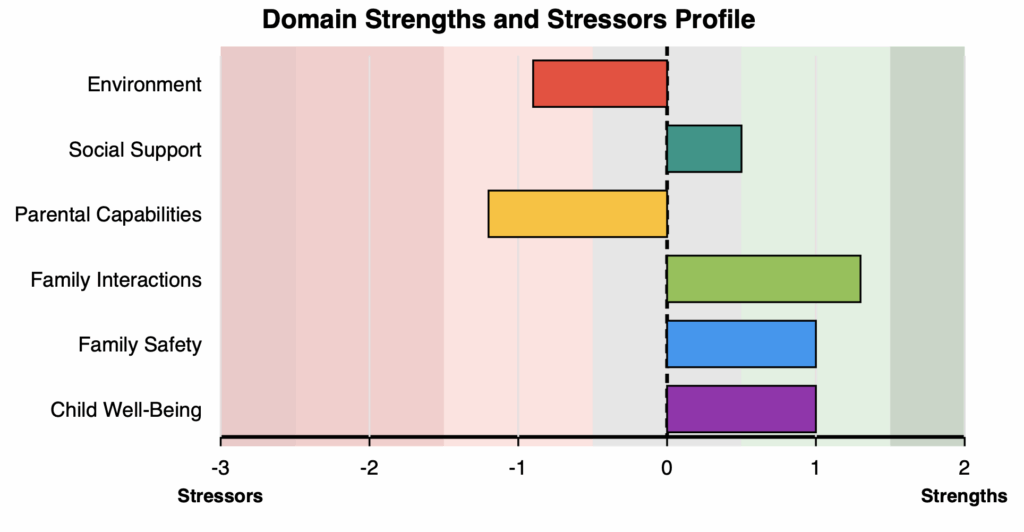
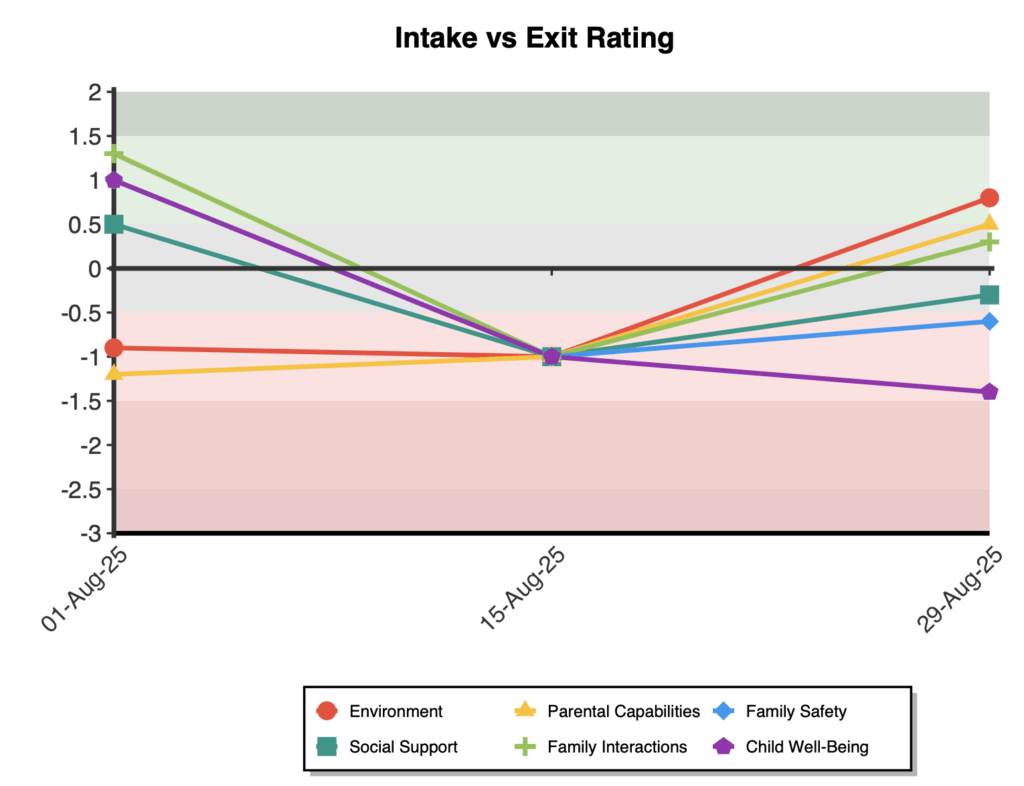
On first administration a two-way horizontal bar graph is displayed showing all six domain scores ranging from -3 to +2. On multiple administrations a line graph of all domains is shown to track scores over time.
The SAS demonstrates robust construct validity as a measure of family functioning within child protection contexts. Initial validation research by Berry et al. (2003) established the scale’s ability to differentiate between families experiencing different forms of maltreatment, supporting its discriminant validity. The instrument showed particular sensitivity in identifying families where physical abuse was the primary concern, suggesting strong criterion validity for this specific risk factor.
Reliability analyses have yielded consistently high internal consistency coefficients across the scale’s domains. Berry et al. (2003) reported alpha values ranging from α = .88 to .91 in their validation sample of 53 families receiving services from a metropolitan child welfare agency. These findings indicate excellent internal reliability, suggesting that items within each domain coherently measure their intended constructs. The high internal consistency values support the scale’s use as both a comprehensive assessment tool and a domain-specific measure of family functioning.
The SAS’s factor structure aligns with its theoretical six-domain framework, though limited published factor analytic studies are available. The conceptual organisation into Environment, Social Support, Parental Capabilities, Family Interactions, Family Safety, and Child Well-Being domains reflects established child welfare assessment frameworks and has demonstrated clinical utility in practice settings. This structure enables practitioners to develop differentiated intervention plans targeting specific areas of family functioning whilst maintaining a holistic perspective on family dynamics.
Regarding sensitivity to change, Berry et al. (2003) found that the SAS successfully detected improvements in family functioning over the course of intervention. This responsiveness to change supports the scale’s utility as an outcome monitoring tool, enabling practitioners to track family progress and adjust interventions accordingly. The ability to capture both deterioration and improvement in family circumstances makes the SAS particularly valuable for ongoing case management and decision-making about service provision.
Normative data for the SAS remains limited, with the primary validation study providing initial benchmarks from a child welfare population. Berry et al. (2003) examined 53 families actively receiving child protection services, though specific means and standard deviations for total and domain scores were not comprehensively reported in the published literature. The scale’s bipolar rating system, ranging from -3 (serious stressor) to +2 (clear strength), provides an intuitive framework for interpretation, with scores around zero representing adequate or typical functioning within community norms. Further research with larger and more diverse samples would strengthen the normative base for the instrument.
The scale’s clinical utility is enhanced by its comprehensive coverage of factors relevant to child protection decision-making. Unlike many risk assessment tools that focus primarily on deficits, the SAS’s balanced approach to identifying both strengths and stressors aligns with contemporary best practices in child welfare that emphasise family preservation and strength-based interventions where appropriate.



