The Reflective Practice Questionnaire – Extended (RPQ-E), developed by Priddis and Rogers (2018) and refined by Rogers and colleagues (2024), is a 30-item self-report measure that assesses frequency of work-related reflective practice and associated work related qualities such as confidence, stress and work satisfaction. The RPQ-E has been used by a wide array of professionals, such as health, education and retail workers, however this implementation is focussed on the questionnaire’s utility among mental health professionals. It is a useful tool for therapists, counsellors, psychologists and other mental health professionals to reflect on their relationship to work.
Reflective practice is the tendency to actively reflect upon the thoughts and actions that occur when working with clients. These reflections may be relational (e.g., considering how one’s own thoughts and feelings influence the interaction, or observing the client’s behaviors during the interaction) or task-focused (e.g., evaluating the strategies and techniques used). Reflections can occur during the interaction itself (reflection-in-action) or afterwards (reflection-on-action). Higher levels of reflective practice are associated with professional development, improved client outcomes, and adaptive responses to workplace challenges.
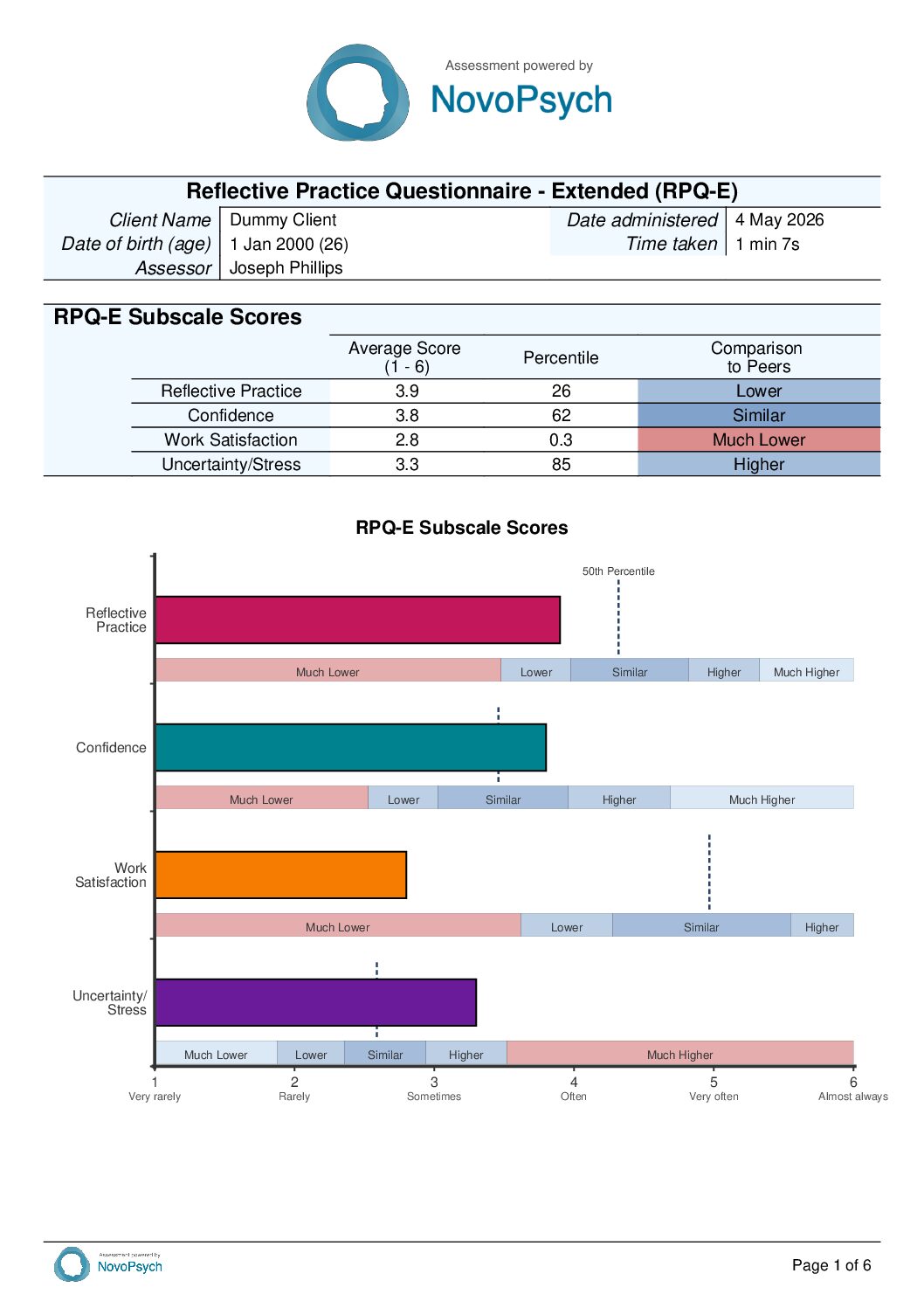
The RPQ-E has four subscales:
RPQ-E Example Item

Among mental health practitioners reflective practice is a core professional competency. Practitioners who engage in frequent reflective practice tend to be more attuned to relational dynamics in their work, more responsive to client needs, and more able to adapt their approach when something is not working. Higher reflective practice is associated with improved client outcomes, accelerated professional development, and more adaptive responses to workplace challenges (Mann, Gordon, & MacLeod, 2009). For the clinician, regular reflection supports ongoing skill refinement and helps surface blind spots that might otherwise persist unchallenged. This implementation of the RPQ-E is designed as a clinician self-assessment tool or in supervision and training mental health professionals.
Practitioners can complete the measure on themselves or as part of supervision. The results profile provides information about how the respondent sits relative to peers and can be helpful identify targets for professional development.
Each of the four subscales are presented as the average of its likert rated items, with 1 representing Very Rarely and 6 being Almost Always. There is no total score for the RPQ-E; each subscale is interpreted independently as part of a professional profile.

The four subscales and their score ranges are:
Each subscale score is converted to a percentile rank compared to the sample of mental health practitioners who self-administered the RPQ-E. The RPQ-E is used as a self-assessment tool by practitioners reflecting on their own professional functioning. In this context, peer comparison provides a useful interpretive frame: a percentile of 50 means the respondent scored higher than 50% of their peers (i.e., at the peer average); a percentile of 90 means the respondent scored higher than 90% of their peers.
The interpretive direction of high and low percentiles depends on the subscale. For Reflective Practice, higher percentiles indicate more frequent engagement in reflective practice, generally a desirable professional disposition. As with any norm-referenced measure, both ends of the distribution can be clinically informative depending on the practitioner’s context.
Descriptor categories are anchored to percentile bands derived from the NovoPsych reference sample (N = 194). The same five bands apply across all four subscales and use a peer-comparison framing appropriate for clinicians self-assessing.


The combinations below have not been independently validated as distinct clinical profiles. They are offered as patterns that may add interpretive insight beyond what any single subscale conveys, and should be treated as hypotheses to explore in supervision or reflection.
The original Reflective Practice Questionnaire (RPQ) was a 40-item measure with 10 subscales (Priddis & Rogers, 2018). Rogers and colleagues (2024) conducted an exploratory factor analysis with 501 Australian university students in paid employment to streamline the measure. This reduced the 30 items used in the RPQ-E. The first 10 items of the RPQ-E can also be administered as a brief version of the RPQ-E, with a focus of reflective practice.
Internal consistency for the four RPQ-E subscales ranged from adequate to strong in the development sample (N = 501, Australian university students in paid employment): Reflective Practice demonstrated strong internal consistency (α = .89), Confidence was strong (α = .87), Work Satisfaction was strong (α = .86), and Uncertainty/Stress was adequate to strong (α = .83). Gabrielsson and colleagues (2022) reported comparable internal consistency in a sample of post-registration specialist nursing students, with subscale alphas ranging from adequate (α = .72) to strong (α = .85) (Sadusky & Spinks, 2022).
The RPQ-E has a four-factor structure established through exploratory factor analysis (Rogers et al., 2024). Reflective Practice and Confidence emerged as strong, well-defined factors. Uncertainty/Stress as moderately strong, while Work Satisfaction explained reflective practice the least. The authors note scope for further subdivision of the Confidence and Uncertainty/Stress factors into sub-components (General Confidence and Communication Confidence; Stress and Uncertainty), though this has not been independently validated as a separate factor structure.
Discriminant validity was supported by weak correlations between RPQ Reflective Practice and two general self-reflection measures: the Self-Reflection and Insight Scale (SRIS; r = .32) and the Rumination-Reflection Questionnaire (RRQ; r = .23) (Rogers et al., 2024). These weak associations indicate that work-specific reflective practice, as measured by the RPQ-E, is distinct from broader self-reflective tendencies.
Inter-subscale correlations followed expected patterns: Reflective Practice was weakly to moderately positively correlated with all three other subscales: Work Satisfaction (r = .30), Uncertainty/Stress (r = .26), and Confidence (r = .17). Notably, the correlation with Uncertainty/Stress is slightly stronger than with Confidence, suggesting that practitioners who reflect more frequently are also somewhat more attuned to professional uncertainty and stress, possibly because reflection brings greater awareness of complexity and limits to one’s competence (elevated Reflective Practice combined with elevated Uncertainty/Stress may indicate ruminative rather than constructive reflection). Confidence was negatively correlated with Uncertainty/Stress (r = -.40) and positively correlated with Work Satisfaction (r = .21). Uncertainty/Stress was negatively correlated with Work Satisfaction (r = -.22).
Validity was demonstrated through industry comparisons (Rogers et al., 2024), comparing professionals in health, education, retail and accommodation/food services. Average reflective practice scores were significantly highest for health and education professionals(η² = .06). Work satisfaction showed substantial industry differences (η² = .19), with health and education industries scoring higher than retail and accommodation/food. These patterns are consistent with the expectation that reflective practice would be more frequent in professions where it is taught and encouraged.
Multiple studies using the original RPQ have documented score changes following structured interventions, including reflective practice programs, supervision training, and medical education courses (Da Silva et al., 2022; Khalil & Hashish, 2022; Van Winkle et al., 2021, 2022). Most of these studies used the reflective practice subscale from the original RPQ, which maps directly to the RPQ-E Reflective Practice subscale. Sensitivity to change evidence for the Confidence, Uncertainty/Stress, and Work Satisfaction subscales is limited.
Percentile norms for mental health professionals were derived from a reference sample of 194 practitioners who self administered the assessment and consented for data to be used for psychometric research in May 2026. The majority of this sample were practising psychologists (54%), with 14% counsellors, 8% therapists and 24% psychotherapists, social workers, nurses, occupational therapists or other allied health professionals. The median years of professional practice was 9.5, with 26% being early in their career (3 years or less).
The mental health practitioner sample were invited to self-administer the RPQ-E in the context of a registering for professional development on reflective practice, so the sample likely consists of practitioners who are interested in reflective practice and therefore probably score higher than typical. Peer comparisons should be interpreted in this context as well as in consideration of social-desirability bias.
Reference sample averages and spread are: Reflective Practice (M = 4.38, SD = 0.70), Confidence (M = 3.54, SD = 0.82), and Work Satisfaction (M = 4.88, SD = 0.90), Uncertainty/Stress (M = 2.69, SD = 0.71). Of note, confidence was significantly correlated with years of professional experience. Reflective practice itself was correlated with each of the other three subscales in expected directions: individuals who engaged in Reflective Practice more often also indicated higher work satisfaction (r = .36), higher confidence in their performance (r = .31), and slightly lower levels of stress and uncertainty (r = −.14).